NeuroDiseaseMonitor
The NeuroDiseaseMonitor is the first database that comprises comprehensive, accurate and long-term data on the characteristics of dementia and Parkinson’s disease. The aim of the monitoring is to better understand the diseases and its temporal and spatial extent as well as the risk factors and to enable a long-term observation of the disease development. It is built up and maintained by the German Center of Neurodegenerative Diseases (DZNE).
Why Monitoring Neurodegenerative Diseases?
Neurodegenerative diseases, especially dementia will be one of the leading medical and societal challenges of ageing populations.
Cognitive decline in higher ages is not a newly discovered phenomenon, but it is growing in importance, as an increased number of people reach higher ages, in which the incidence of dementia and Parkinson’s disease are becoming more likely. So, neurodegenerative diseases are not any more rare diseases and there is a high and growing need of monitoring dementia and Parkinson’s disease to fill the gap in epidemiologic research in Germany.
Therefore, it is required to have a timely, comprehensive and accurate monitoring system, to enable a deeper research on causes, determinants and trends of neurodegenerative diseases. That is important in many aspects and different subgroups of the population will benefit directly and indirectly of the monitoring:
Researchers will have access to reliable data, which they can use to provide better estimates, to promote research to risk factors and to identify differences among demographic characteristics. Next to that they can use the different data to estimate future developments of the number of affected persons. The forecasts are particularly important for policy makers’ of social and medical service provision in the near and far future.
In addition, economic actors, for example pharmaceutical firms, medical engineering or care service providers are interested and in need of data for their planning. Furthermore, health agents like physicians, nurses, care givers and, last but not least, the patients themselves and their relatives will profit from the monitoring.
By the year 2050 the number of people with dementia will increase by two to three million persons. The quite huge range of one million affected persons is due to the uncertainty of future developments. There are still open questions, for example, how life expectancy with or without neurodegenerative diseases will develop or how possible future preventive interventions take effects.
The NeuroDiseaseMonitor builds the basis for an advancing, to be updated and long-term observation of the development of dementia and Parkinson’s disease, which will be highly relevant for future generations of every age.
Hier finden Sie unsere Nutzungsbedingungen und die Erklärung zum Datenschutz zum download.
Zur Ansicht der Datei wird der Adobe Reader benötigt.
Using Claims Data of German Health Insurers to Monitor Neurodegenerative Disease (ND)
There are several approaches and methods for identifying ND, ranging from the very detailed and deep ascertainment of the pathology in an individual, to a brief and broad standard assessment emphasizing individual functioning (Launer 2011). These measurements not only differ in their validity and reliability, but may also lead to different estimates of the prevalence and incidence of ND. The purpose of the research being conducted determines the assessment approach. If the aim is to better understand the etiology of ND, to identify risk factors, and to predict who will suffer from the disease based on an individual’s specific characteristics, then a deep phenotyping based on neuropsychological tests, biomarkers, and MRT and PET scans is necessary. If, however, the aim is to determine the prevalence and incidence of the disease for the purposes of general health planning and related activities, a broad approach is sufficient (Launer 2011). As detailed phenotyping is cost-intensive, usually only a limited number of individuals are enrolled in these studies. Thus, the estimates of prevalence and incidence suffer from large standard errors and are imprecise, particularly at older ages. The broad approach to assessing dementia permits the inclusion of large numbers of people, sometimes even the total population, and provides a better understanding of the occurrence of the disease; it cannot, however, provide information about etiology.
Data source
The NeuroDiseaseMonitor is based on newly available and comprehensive health claims data from all German statutory health insurance funds (SHIF) provided by the German Institute of Medical Documentation and Information (DIMDI). The database covers 70 million persons, which is approximately 86% of the general German population and comprises, in addition to other components, diagnostic data from the inpatient and outpatient sectors. As of now, data are available for the period 2009–2013; however, the NeuroDiseaseMonitor will be updated regularly as new data become available.
Study participants
The cohorts upon which the calculations are based (denominator) consist of the German population from the respective years (2009, 2010, 2011, 2012, or 2013) aged 65 and above who live in their community or in nursing homes. They are included independent of whether they received medical treatment or not. Persons who survived the respective year had to be insured for at least 360 days in order to cover the entire time at risk for seeking medical attention. Persons who moved abroad or who switched to a private insurance plan in the year of analysis are not included. However, at this age range, the number of people switching to private health insurance is negligible. According to these criteria, we arrived at a cohort size of about 14.5 million insured persons (6 million males, and 8.5 million females) for each year.
Case ascertainment of Dementia and Parkinson’s disease
Diagnoses are based on the International Classification of Diseases, Tenth Revision (ICD-10) in the inpatient and outpatient sectors. Dementia corresponds to the ICD-10 codes G30, G31.0, G31.82, G23.1, F00, F01, F02, F03, and F05.1. Parkinson’s disease was defined by the ICD-10 codes G20.0, G20.1, G20.2, and G20.9. To account for false positive diagnoses of the true occurrence of dementia, we developed a validation procedure. Only valid dementia or Parkinson’s disease diagnoses were considered. A diagnosis was found to be valid if (1) the diagnosis was internally marked as “verified” in the outpatient sector or as “main diagnosis” or “secondary diagnosis” in the inpatient sector, and (2) if a patient received a confirmative diagnosis in the respective year (2009–2013). Diagnoses of persons who died stem from the calendar year before death, as diagnoses for these persons were not available in the year of death.
Indicators
At the moment, the NeuroDiseaseMonitor contains yearly information on period prevalences of dementia and Parkinson’s disease by men and women and five-year age groups for Germany as a whole. Yearly five-year-age- and sex-specific prevalences were estimated by dividing all valid dementia or Parkinson’s disease cases by the number of insured persons in a given year and are expressed as dementia or Parkinson’s disease cases per 100,000 persons.
The information about prevalence is provided in two forms: first, age-specific prevalences are presented in the online version of the NeuroDiseaseMonitor; and, second, the prevalences can be downloaded together with the underlying nominator (cases) and denominator (number of persons).
The NeuroDiseaseMonitor also contains the health indicator “disease-free life expectancy” which combines life expectancy with prevalence of dementia or Parkinson’s disease respectively. Here, the number of years of remaining life expectancy at a given age with and without the disease is given, as is the proportion of healthy years out of the total number of years of remaining life expectancy (health ratio).
Limitations
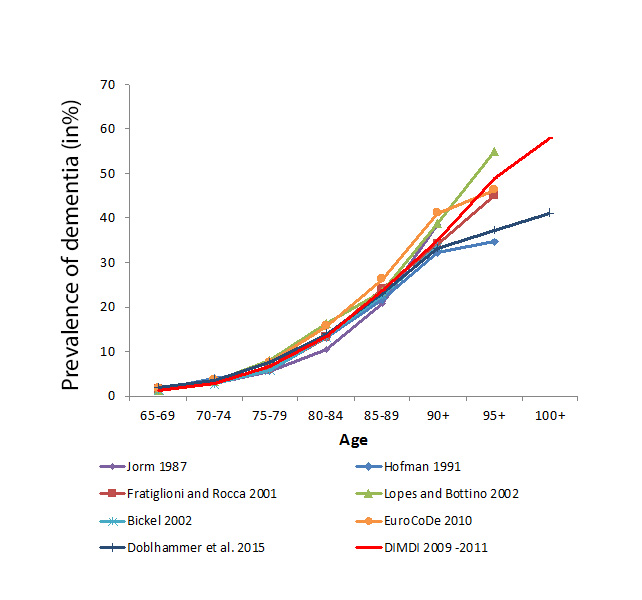
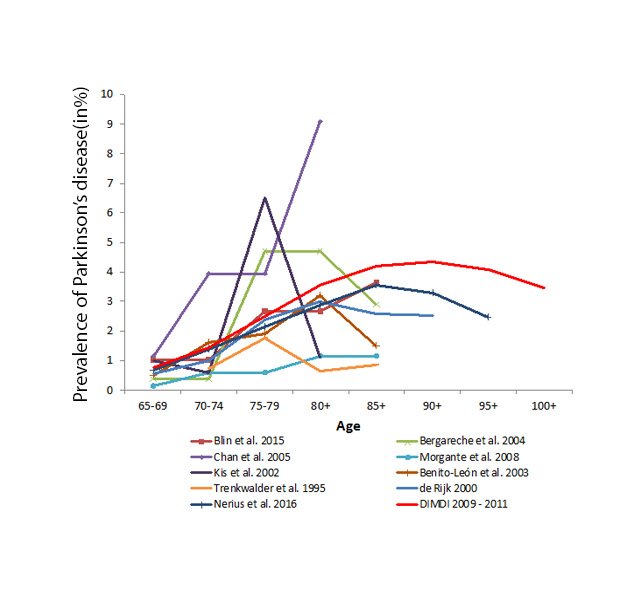
These claims data do, however, have some important limitations. Unlike for population-based epidemiologic and clinical research, there is no connection to the research question at the time of data collection. There are no clinical data on, for example, the severity of the disease; and the validity of diagnoses is not fully given. Furthermore, routine data are subject to legal changes and to international changes in the data-handling procedures of the health insurers. Therefore, an internal validation of the diagnoses is required. At present, there are no options for validating claims data externally, except for comparing the estimated prevalence and incidence with results from other national and international studies. Following the latter approach, German health insurance claims data have been proven to be a suitable source for epidemiologic research, especially for providing a general picture of the occurrence of dementia (Ziegler & Doblhammer 2009; Ziegler 2011; Doblhammer et al. 2012). The following figures compare prevalence and incidence rates based on claims data from health insurers with results from international studies.
References
- Doblhammer, G., Schulz, A., Steinberg, J., Ziegler, U. (2012): Demografie der Demenz. Bern, Verlag Hans Huber, Hofgrefe AG.
- Launer L. J. (2011): Counting dementia: There is no one ‘best’ way. Alzheimer’s and Dementia, 7 (1): 10-14.
- Ziegler, U., Doblhammer, G. (2009): Prävalenz und Inzidenz von Demenz in Deutschland. Eine Studie auf Basis von Daten der gesetzlichen Krankenversicherungen von 2002. Das Gesundheitswesen, 71: 281-290.
- Ziegler, U. (2011). Dementia in Germany: Past Trends and Future Developments. Rostock, Südwestdeutscher Verlag für Hochschulschriften
In the course of the development of the NeuroDiseaseMonitor, the German Center for Neurodegenerative Diseases in Bonn (DZNE) and the PMV Forschungsgruppe, Cologne, organized the workshop "Monitoring Dementia – Towards a Dementia Monitoring System and a Dementia Registry in Germany", which took place on November 17-18, 2011. The aim of the workshop was to discuss the use of registry and health insurance data for the purposes of dementia monitoring.
The workshop brought together experts who have either established a national dementia registry, or are working with registry or health data in the area of dementia and cognitive functioning. The following aspects were discussed:
- Research findings about the prevalence and incidence of dementia in Europe
- Existing population-based data sources that permit epidemiological studies of dementia
- The need for new data sources
- Population-based data from health registries and health insurers
- The contribution of these data to a better understanding of the risk of dementia and the health pathways of dementia patients
- The validity of data from health insurers for the purposes of monitoring trends in dementia
- The creation of a national dementia registry in Germany
- Lessons from the experience of existing dementia registries, as well as of national cancer registries
The DZNE aims at strengthening the interdisciplinary scientific exchange between clinical and population-based epidemiological research. In the course of the Symposium "Neurodegenerative Diseases: New Insights from Registries, Cohorts and Health Care Data", internationally renowned scientists presented their latest research results by using registers, population-based cohort studies, as well as administrative data of health care insurances.The symposium took place in Bonn on April 29-30, 2013.
The working group “Demographic Studies” of Prof. Gabriele Doblhammer at the German Center for Neurodegenerative Disease (DZNE) has organized the “Third Workshop on Monitoring Dementia – New Insights from Health Claims Data, Electronic Medical Records and Population-Based Cohort Studies”, which took place on October 17-18, 2018, in Bonn, Germany.
The aim of the workshop was to discuss the possibilities and limits of the use of health claims data and electronic medical records in dementia research. A particular focus was on the potential of big data and digital data for advancing dementia research.
Researchers from a wide range of scientific disciplines presented and discussed following aspects:
- Causal inference from observational data
- Surveillance of dementia
- Prevalence and trends
- Pharmacoepidemiological analyses
- Big data and digital data in monitoring dementia
- Methodological aspects
- Risk factors and prevention
- End-of-life research
Publications based on German Health Claims Date
- Teipel SJ, Fritze T, Ellenrieder M, Haenisch B, Mittelmeier W, Doblhammer G. Association of joint replacement surgery with incident dementia diagnosis in German claims data. Int Psychogeriatr 2018 Mar 21:1-9.
- Kreft D, Barth A, Fink A, Nerius M, Doblhammer G, Fritze T. Aktueller Stand und Prognose des Krankenhausbedarfs von Personen mit und ohne Demenz in Deutschland. In: Klauber J, Geraedts M, Friedrich J, Wasem J, editors. Krankenhaus-Report 2018: Bedarf und Bedarfsgerechtigkeit. Stuttgart: Schattauer; 2018. p. 193-207.
- Nerius M, Johnell K, Garcia-Ptacek S, Eriksdotter M, Haenisch B, Doblhammer G. The Impact of Antipsychotic Drugs on Long-term Care, Nursing Home Admission and Death among Dementia Patients. J Gerontol A Biol Sci Med Sci 2017 Dec 8.
- Nerius M, Fink A, Doblhammer G. Parkinson's disease in Germany: prevalence and incidence based on health claims data. Acta Neurol Scand 2017 Nov;136:386-92.
- Zhou Y, Putter H, Doblhammer G. Years of life lost due to lower extremity injury in association with dementia, and care need: a 6-year follow-up population-based study using a multi-state approach among German elderly. BMC Geriatr 2016;16:9.
- Gomm W, von Holt K, Thome F, Broich K, Maier W, Weckbecker K, et al. Regular Benzodiazepine and Z-Substance Use and Risk of Dementia: An Analysis of German Claims Data. J Alzheimers Dis 2016 Sep 06;54:801-8.
- Gomm W, von Holt K, Thome F, Broich K, Maier W, Fink A, et al. Association of Proton Pump Inhibitors With Risk of Dementia: A Pharmacoepidemiological Claims Data Analysis. JAMA Neurol 2016 Apr;73:410-6.
- Fritze T, Teipel S, Ovari A, Kilimann I, Witt G, Doblhammer G. Hearing Impairment Affects Dementia Incidence. An Analysis Based on Longitudinal Health Claims Data in Germany. PLoS One 2016;11:e0156876.
- Barth A, Vatterrott A, Zhou Y, Fink A, Doblhammer G. Extremity injuries and dementia disproportionately increase the risk for long-term care at older age in an analysis of German Health Insurance routine data for the years 2006 to 2010. Eur Rev Aging Phys Act 2016;13:9.
- Teipel S, Fritze T, Ovari A, Buhr A, Kilimann I, Witt G, et al. Regional Pattern of Dementia and Prevalence of Hearing Impairment in Germany. J Am Geriatr Soc 2015 Aug;63:1527-33.
- Heneka MT, Fink A, Doblhammer G. Effect of pioglitazone medication on the incidence of dementia. Ann Neurol 2015 Aug;78:284-94.
- Fink A, Doblhammer G. Risk of Long-Term Care Dependence for Dementia Patients is Associated with Type of Physician: An Analysis of German Health Claims Data for the Years 2006 to 2010. J Alzheimers Dis 2015;47:443-52.
- Fink A. Dementia and Long-Term Care – An Analysis Based on German Health Insurance Data. In: Doblhammer G, editor. Health among the Elderly in Germany: New Evidence on Disease, Disability and Care Need. Series on Population Studies by the German Federal Institute for Population Research. 46. Opladen, Berlin, Toronto: Barbara Budrich; 2015.
- Doblhammer G, Fritze T, Teipel SJ. Spatial patterns of dementia prevalence and its vascular risk factors in Germany. In: Doblhammer G, editor. Health among the Elderly in Germany: New Evidence on Disease, Disability and Care Need. Series on Population Studies by the German Federal Institute for Population Research. 46. Opladen, Berlin, Toronto: Barbara Budrich; 2015.
- Doblhammer G, Fritze T. Month of Birth and Dementia Late in Life. KZfSS Kölner Zeitschrift für Soziologie und Sozialpsychologie 2015;67:217-40.
- Doblhammer G, Fink A, Zylla S, Willekens F. Compression or expansion of dementia in Germany? An observational study of short-term trends in incidence and death rates of dementia between 2006/07 and 2009/10 based on German health insurance data. Alzheimers Res Ther 2015 Nov 05;7:66.
- Doblhammer G, Fink A, Fritze T. Short-term trends in dementia prevalence in Germany between the years 2007 and 2009. Alzheimers Dement 2015 Mar;11:291-9.
- Doblhammer G, Fink A, Fritze T, Günster C. The demography and epidemiology of dementia. Geriatric Mental Health Care 2013;1:29-33.
- Schulz A, Doblhammer G. Aktueller und zukünftiger Krankenbestand von Demenz in Deutschland auf Basis der Routinedaten der AOK. In: Günster C, Klose J, Schmacke N, editors. Versorgungs-Report 2012: Schwerpunkt: Gesundheit im Alter. Stuttgart: Schattauer; 2012.
- Doblhammer G, Schulz A, Steinberg J, Ziegler U. Demografie der Demenz. Bern: Verlag Hans Huber, Hofgrefe AG; 2012.
- Schulz A, Doblhammer-Reiter G, Gunster C, Klauber J. Trends of dementia in Germany from 2004 to 2008: Analysis on AOK basis of routine data. Z Gerontol Geriatr 2010 Sep;43:79-.
- Ziegler U, Doblhammer G. Prevalence and Incidence of Dementia in Germany - A Study Based on Data from the Public Sick Funds in 2002. Gesundheitswesen 2009 May;71:281-90.
- Doblhammer G, Ziegler U, Muth E. Trends und Muster in Lebenserwartung und Gesundheit und Prognose der Demenzerkrankungen in Deutschland bis 2050. In: Kumbier E, Teipel SJ, Herpertz SC, editors. Ethik und Erinnerung–Zur Verantwortung der Psychiatrie in Vergangenheit und Gegenwart Lengerich: Pabst Science; 2009. p. 91-108.
Contact
Dr. Anne Fink
Deutsches Zentrum für Neurodegenerative Erkrankungen e.V. (DZNE)
Ulmenstraße 69
18057 Rostock